Current law (Sec. 144E.06) stipulates that ambulance providers perform Emergency Medical Services (“EMS”) in exclusive
operating areas or Primary Service Areas (“PSAs”).
In the 1980s, when PSA’s were established, ambulance providers were granted these permanent service territories
without any direct accountability to the governmental units within those areas and very lax state supervision.
The PSA operating license areas are essentially “owned” by the ambulance provider and they control the transfer
and sale (see Sec. 144E.07) of these service area licenses to other entities.
An ambulance provider license is multi-faceted license with various requirements. The PSA is specified in the
license.
The Emergency Medical Services Regulatory Board (EMSRB), is the state’s EMS regulatory agency that oversees
and issues ambulance licenses. The EMSRB has been less than effective and its close ties with the ambulance
service industry may create conflict of interest.
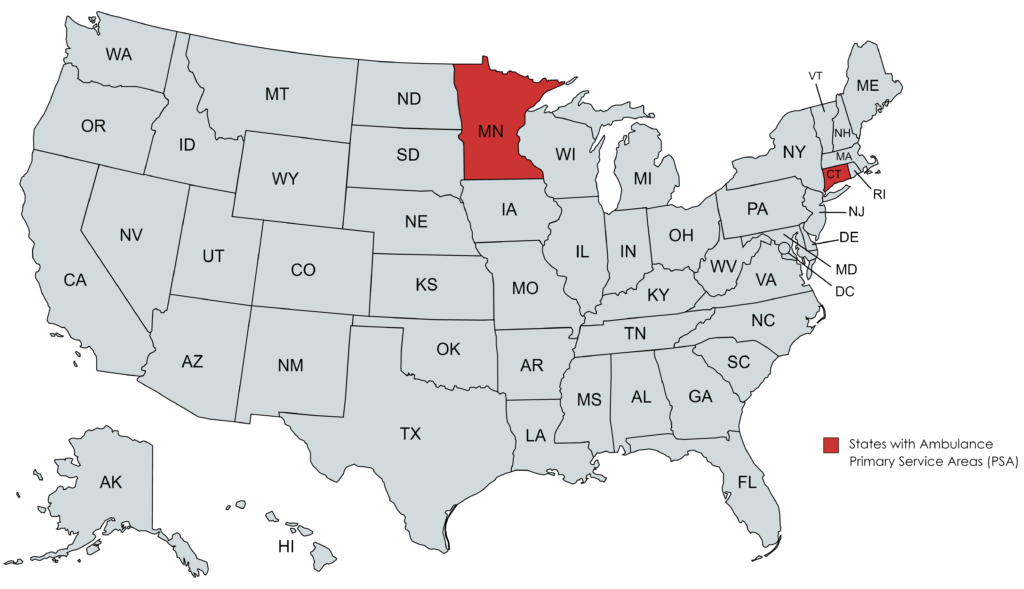
A nationwide comparison
Minnesota’s PSA structure is very unique. So unique in fact that the only other state that has a relatively comparable structure is Connecticut (population 3.6 million).
Recommendations
- Modify existing PSAs to correspond with local governing units (“LGU”) lines. The LGU would be given decision-making authority regarding ambulance service providers during the existing renewal timeline. Any change in ambulance service provider (including “name change” and buy-outs) would trigger an immediate license renewal process.
- Require performance standards be set during the license renewal process. The report must include, but is not limited to the following:
- Number and type of calls by LGU;
- Amount of fees for services to be posted publicly by the ambulance service for the fees charged in the local unit of government territory;
- Response time and mode (emergent versus non-emergent) from 911 until ambulance arrival with required staff;
- Transport percentage by local unit of government;
- Transport destinations by local unit of government;
- Number of ambulances staffed by time of day and day of week by local unit of government (how many ambulances were stations in that local unit of government throughout the quarter); and
- Mutual aid given and received.
- Quality assurance metrics reviewed over that quarter (what clinical and operational items were reviewed by quality assurance staff)
- Consistent definitions of “response time” and “quality of care”.
- Require a quarterly report to be delivered to the local units of government with oversight authority of the EMS in that PSA.
Frequently Asked Questions (FAQs)
Local Control and PSAs
In the majority of cities and towns across the state of Minnesota, local units of governments have little or no voice in who provides ambulance service to their communities.
The 2022 Emergency Ambulance Service Evaluation Report by the Office of the Legislative Auditor specifically states, “We recommend that the Legislature retain primary service areas. However, it should restructure how they are created, modified, and overseen.”
No. We simply believe that all local units of governments in Minnesota should have input and control over who provides ambulance service to their community. There are many different types of ambulance service models that exist across the country, including hospital based, independent (including both for- and non-profit services), as well as government operated agencies (e.g. fire-based ambulance services). Only a quarter of fire departments in the United States provide ambulance service.
The decision of a local unit of government (whether a city, town, or county) to provide ambulance services (whether through the fire department or another governmental body) is something that should rest with the elected body of that local unit of government. The Minnesota State Fire Chiefs Association (MSFCA) has not, and is not, advocating that this decision be the local fire chief’s – it is truly something that should be left up to the local unit of government (who were elected by their constituents to represent them).
Yes. This is actually quite common. There is no requirement when an ambulance provider transfers or sells their PSA for them to solicit public feedback or input. A local unit of government has little influence or control in an ambulance provider selling their PSA.
Other than Minnesota, the only other state that has a similar ambulance PSA law is Connecticut.
In fact, Minnesota and Connecticut are the only two states that explicitly require a state regulatory authority to establish service areas and assign a single ambulance service provider to each one. Connecticut’s system is also significantly more robust than Minnesota’s system, as Connecticut affords to local communities and regional EMS entities a mechanism through which they can petition the state agency tasked with allocating EMS service areas to revoke an ambulance service provider’s service area assignment when necessary to protect public health and safety.
Source: Improving Emergency Medical Services in Minnesota: A Legal Analysis of Minnesota’s EMS Statutes and Regulations
No. Local control means that the local unit of government has a say in who provides ambulance services to their community (just like local police, fire, and public works services), but it is not an edict that the local fire department takes on providing ambulance services. The Minnesota State Fire Chiefs Association (MSFCA) and its allied partners would strongly recommend that local elected officials and public safety leaders conduct a full needs analysis and develop a comprehensive plan if they intend on assuming ambulance transport responsibilities. Such a plan should factor in the impact on existing services.
There is no quantifiable or factual data to support this assertion, and frankly is a fear tactic being used by some providers to maintain the status quo in Minnesota. In fact, according to the 2022 OLA Emergency Ambulance Services Evaluation Report, the State has very little oversight over existing PSAs and specifically recommends that, “[t]he Legislature should establish a process through which local units of government have input into which services provide ambulance care and transportation in their areas.”
Allowing local units of government to have local control over who provides ambulance service to their community will benefit all of Minnesota. A small, rural township should have the same rights and privileges’ to represent their community and their constituents (who voted them into office) just as much as larger “metro” communities.
Local elected officials are trusted by their constituents to represent their interests – above all, public safety. Local leaders can make decisions about their police services, fire departments, public works, trash collectors, golf courses, liquor stores (in some areas), and even manage cable franchising agreements. There is no reason why they can’t be trusted to make decisions about their ambulance services. We trust our local elected leaders.